Address
3rd Floor, HYGEIA Hospital, 4 Erythrou Stavrou Street, 15123 Athens
Appointment
Daily 8am- 3pm
The Ear
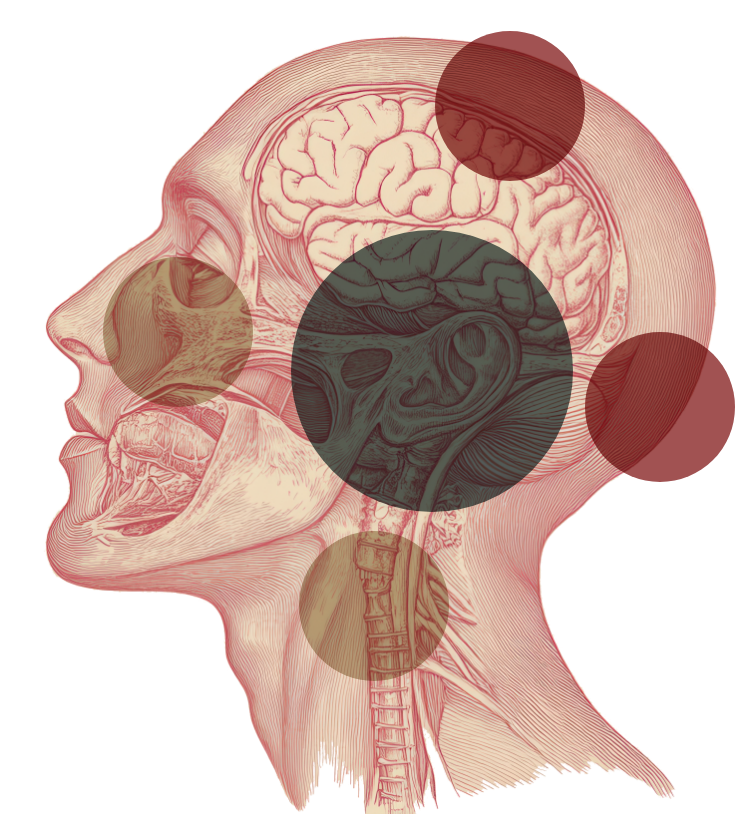
The ear consists of the outer, middle, and inner ear. Sound travels through the outer ear to reach the eardrum, causing it to vibrate. This vibration is then transmitted through three very small bones (ossicles) located in the middle ear. These three bones are called the malleus, incus, and stapes, forming the auditory chain. The sound vibration then enters the inner ear, which consists of a bony structure filled with fluid in the shape of a snail shell (cochlea). The fluid in the inner ear creates waves that stimulate the sensory nerve cells of the ear. This generates nerve signals that are transmitted to the brain and perceived as sound.
What is the mastoid bone?
The mastoid bone is the part of the skull located just behind the outer ear. It is made up of air-filled cavities, the largest of which is called the antrum. This space connects directly to the middle ear, which also normally contains air. For this reason, diseases of the middle ear can spread to the mastoid bone.
When is mastoidectomy needed?
A mastoidectomy—surgery on the mastoid bone—may be necessary when an infection in the middle ear spreads into the mastoid bone. This usually occurs when skin from the external auditory canal grows behind the eardrum and develops in the middle ear space, creating a chronic infection. This condition is known as cholesteatoma.
Cholesteatoma may initially cause chronic ear discharge (otorrhea) and partial hearing loss. Over time, as it grows in layers and forms a sac, it can erode the walls and contents of the middle ear and lead to more serious problems, such as:
further hearing loss (due to ossicle erosion)
vertigo (labyrinth erosion)
facial paralysis (facial nerve erosion)
headaches or even coma (if it erodes the skull base and causes perimeningeal infections)
The only effective way to remove a cholesteatoma is through mastoidectomy.
How is a mastoidectomy performed?
The surgery is performed under general anesthesia. There are different surgical techniques (e.g., atticotomy, modified or radical mastoidectomy), depending on the size of the cholesteatoma and the surgeon’s preference. It takes between one and three hours and involves an incision either above or behind the ear. The mastoid bone—covering the infected cholesteatoma—is removed along with the cholesteatoma. This inevitably creates a cavity, which is usually reconstructed during the procedure using healthy (non-infected) surrounding tissue (bone, cartilage, muscle). At the end of the surgery, an antibiotic-soaked strip (packing) is placed in the ear to aid healing.
How painful is the surgery?
The ear may be sore for a short time after surgery, but this is temporary and can be effectively managed with painkillers.
How successful is the surgery?
Success rates, defined primarily by achieving a “dry” ear, are over 80% in experienced hands. In some cases, hearing may also improve if the ossicular chain in the middle ear is restored.
What are the possible complications?
As with any surgery, there are always potential complications that the patient should be aware of. That said, serious complications from mastoidectomy are rare.
Hearing loss: In a small number of cases, hearing may worsen if the inner ear is damaged either during surgery or due to the extent of the cholesteatoma.
Vertigo: If it occurs, it is usually temporary, lasting only a few hours post-op. Rarely, it may persist longer.
Tinnitus: Ringing in the ear may rarely occur, especially if hearing has deteriorated.
Facial weakness/paralysis: The facial nerve, which controls facial movement, runs through the ear. If injured, it may cause weakness on one side of the face. This is very rare in experienced hands and with the use of nerve monitoring during surgery. Even if it does happen, it is usually temporary.
What happens after surgery?
Usually, the patient returns home the day after surgery, once the head bandage is removed. Stitches are removed 5–7 days later. The antibiotic packing remains in the ear for about 2 weeks. Some drainage of fluid or blood is expected and not concerning.
The ear and wound must be kept dry for a few days to prevent infection.
Sick leave for about one to two weeks is typically needed.